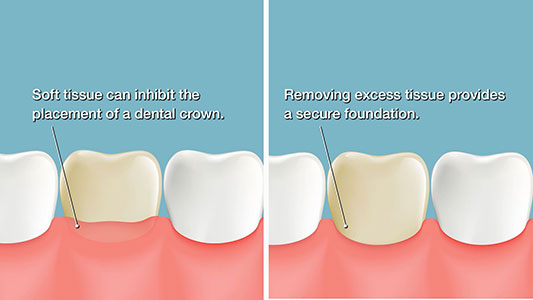
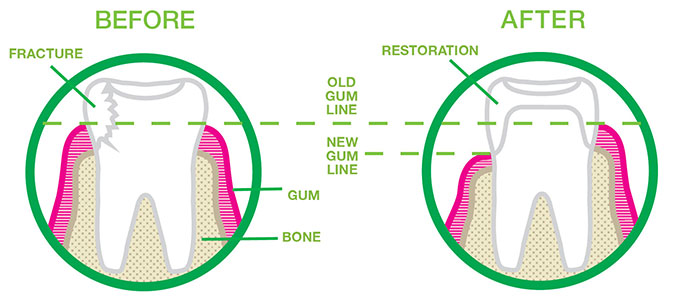
Crown lengthening is a dental procedure performed by Dr. Hawryluk to help restore broken down teeth.
There are many causes for considering crown lengthening. Commonly, the procedure exposes a greater amount of tooth structure to restore the tooth with a dental crown. Other indications to crown lengthen include accessing cavities below the gum, tooth perforations, and treating aesthetic disproportions such as “gummy smiles”. Please note we have defined words marked in (*) at the end of this article.
The concept of Biologic width is key to the crown lengthening procedure. It is the natural length between the base of the gum sulcus and the height of the alveolar bone (*). The gingival sulcus is a small crevice between the enamel of the tooth crown and a junctional epithelium(*) at the crevice base. From the crevice base to the height of the jawbone is about two mm. More specifically, biologic width is the length established by “the junctional epithelium and connective tissue attachment to the root surface” of a tooth. In other words, it’s the height between the alveolar bone crest and the deepest part of the gingival sulcus. It is essential to keep this distance in mind when making dental crowns since we need to appreciate the natural design of the gum tissue to avoid detrimental outcomes.
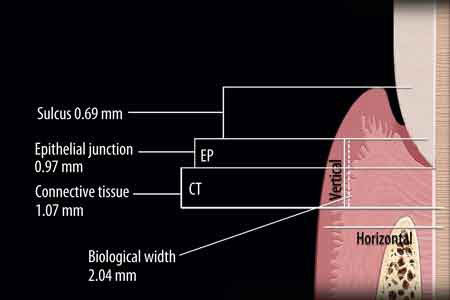
The biologic width varies per individual and is generally between 0.75-4.3 mm. The mean biologic width is 2.04 mm, of which 1.07 mm is connective tissue attachment, and another about 0.97 mm is the junctional epithelium. Since it is impossible to precisely restore a tooth to the upper edge of the junctional epithelium, we sometimes resect enough bone to have 3mm between the crown margin and the crest of the alveolar bone.
If a dentist does not make crowns to these specifications, the biologic width is ‘violated,’ and three main issues can arise:
- Unpredictable loss of alveolar bone.
- Chronic inflammation of the gums.
- Chronic pain.

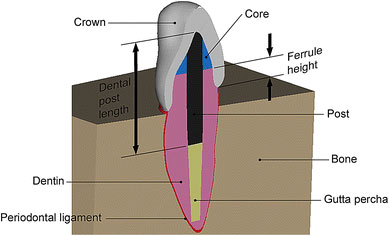
Crown lengthening should create a 2mm tooth height to facilitate a ferrule effect. A ferrule is part of a porcelain crown that surrounds the external dimension of residual tooth structure, not unlike the metal bands around a barrel. Therefore, sufficient vertical height of tooth structure that the future crown will grasp is needed to facilitate a ferrule effect of the future dental crown. In addition, an adequate ferrule reduces fracture incidence in teeth that have had root canals.
The crown lengthening procedure must maintain an acceptable tooth crown to root ratio. The alveolar bone surrounding a tooth also surrounds an adjacent tooth, and resecting bone for a crown lengthening treatment will effectively damage the bony support of neighboring teeth to some extent and unfavorably increase the tooth crown-to-root ratio. Additionally, it is almost impossible to regain it to previous levels after removing bone. Finally, if a patient wants an implant placed in the future, there might not be enough bone in the region after completing a crown lengthening procedure. Dr. Hawryluk always considers this when deciding the best treatment course with you.

When crowning lengthening, Dr. Hawryluk first makes an apically repositioned flap(*) and contours the bone. Next, Dr. Hawryluk designs the flap to place the tissue lower than its original position, exposing more tooth structure. As we mentioned above, we must respect the biological width when doing this procedure.

In general, Dr. Hawryluk must expose at least four mm of sound tooth structure during the procedure. This amount allows for the accumulation of ‘”supra-crestal” soft tissues, covering 2– 3 mm of the exposed root structure, leaving 1–2 mm of exposed tooth structure. Also, we need to account for the tendency of gum tissues to bridge abrupt changes in the contour of the bone crest. Therefore, we sometimes need to do the procedure around the problem tooth and at the adjacent teeth to reduce the bony profile gradually. Consequently, we must watch we don’t lose too much attachment tissue when accomplishing crown lengthening. Also, keep in mind, for esthetic reasons, symmetry of tooth length must be maintained between the right and left sides of the dental arch. Therefore, it may call for even more teeth in the surgical procedure in some situations.
The technique involves Dr. Hawryluk making a reverse bevel incision using a scalpel. He guides the initial incision by preoperative planning, and he bases it on the amount of tooth structure we want to expose. The beveling incision usually follows a scalloped outline. Dr. Hawryluk then raises the tissue to expose the root surfaces. Next, he elevates the flap enough to be able later to reposition the soft tissue. Next, Dr. Hawryluk performs any bone recontouring using a rotating round bur and copious water spray. Recontouring should aim to mimic the ordinary form of the alveolar bone but at a more apical level. Following contouring, the flap is repositioned to the newly recontoured alveolar bone crest level and secured in position.

Sometimes orthodontic forced eruption is done in conjunction with crown lengthening. It is non-invasive, does not damage or remove the bone, and can be cost-effective. First, the dentist extrudes the tooth using light orthodontic force. Treatment time is usually a few months. The tooth and bone will move in unison if the dentist applies moderate forces. The amount we must extrude needs to be a distance equal to or slightly longer than the portion of sound tooth structure that needs exposing. Once stabilized, Dr. Hawryluk will do the crown lengthening to the required tooth structure. Adjacent teeth hard and soft tissues should remain unchanged to restore aesthetic proportions correctly. Dr. Hawryluk recommends forced tooth eruption where crown lengthening is required and where we must preserve attachment and bone from adjacent teeth.

We hope you have enjoyed our article; thank you for reading!
Glossary
- Alveolar bone: The part of the jawbone containing the tooth sockets.
- Junctional epithelium: The portion of the gums that attaches to the tooth’s enamel.
- Apically positioned flap: A procedure involving pulling the tissue away from the teeth to treat the roots and jawbone directly.
Reference:
https://en.wikipedia.org/wiki/Crown_lengthening
Ingber, Jeffrey; Rose, LF; Coslet, JG (1977). “The Biologic Width – A concept in periodontics and restorative dentistry.” Alpha Omegan.
Nevins M, Skurow HM (1984). “The intra-crevicular restorative margin, the biologic width, and the maintenance of the gingival margin.” Int J Perio Rest D.

- Sleep Dentistry: Enhancing Comfort and Care During Dental Procedures - July 11, 2024
- The Revolutionary Injection Molding Technique for Composite Veneers - June 27, 2024
- Why Are Third Molars Called “Wisdom Teeth”? - June 19, 2024