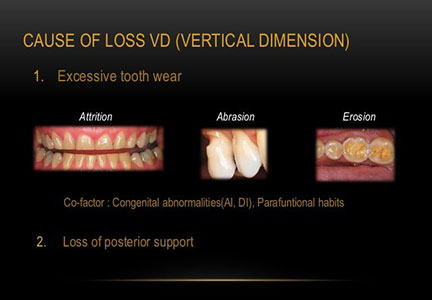
Bite collapse is a dental circumstance distinguished by a change in the configuration of the patient’s facial features, teeth, and jaw function because of tooth loss or severe wearing down of the teeth.
We also call it loss of vertical jaw dimension. St Lawrence Dentistry does treatments to open the bite back up to “restore the vertical jaw dimension” We had already written one blog on this topic before, and the response was phenomenal. The article expands on this topic. When have included a glossary at the end of the blog for the lesser-known terms. We have these marked by a (*) in the article.
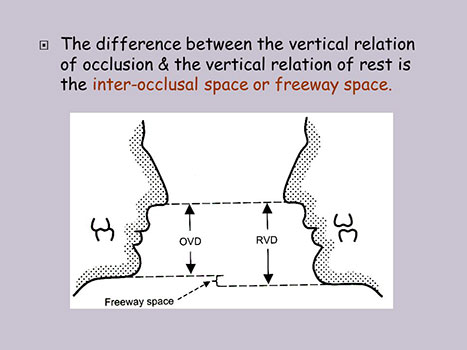
There are few definitions to understand to comprehend how we can change the vertical dimension of one’s jaw. The vertical dimension of speech is the distance measured between two selected points when the occluding members are closest during speech. The vertical dimension of occlusion is the span between two designated anatomic marked points (usually one is the tip of the nose and the other on the chin) when in maximal jaw closure. When considering opening vertical dimensions for a patient, we live between these two measurements. If the dentist opens up vertical dimension too much, the patient can be “robbed” of “freeway space” and create all sorts of trouble.
Interocclusal rest distance is between the rest vertical and the occlusal vertical. This term is also called interocclusal rest space, and Centric occlusion is the occlusal position of opposing teeth when the lower jaw is in centric relation. It may or may not coincide with the maximal jaw-closing position. It’s the tooth contact when the jaw closes in a centric relation movement. Centric relation is an upper and lower jaw relationship independent of tooth contact. In it, the condyles(*) articulate in an anterior-superior position against the posterior slopes of the articular eminences(*). There is a restriction of the mandible to a pure rotary movement in this position. However, the patient can make vertical, lateral, or protrusive movements from this unstrained position.
We generally restore patients to centric relation when making a vertical dimension change. When doing so, we always have to watch out for “compensatory eruption” – a condition defined by teeth shortening and vertical movement caused by grinding and tooth wear. It is nature’s way to keep teeth in contact when worn. Therefore, as we wear our teeth, they well supra erupt into occlusion.
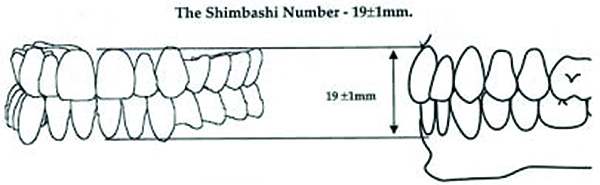
A helpful tool when assessing if your teeth vertical dimension is lost is the “Shinbashi measurement”. It refers to the distance between the cementoenamel junction (*) of the upper and lower central incisors. A class I occlusion (*) usually is 18-19mm. We use this measurement as a reference. When this measurement is changed, we suspect a potential vertical dimension loss (instead of compensatory anterior teeth eruption).
There are a few things to know as a frame of reference when planning comprehensive dental rehabilitation. First, males generally show far less tooth structure than females (1.91mm versus 3.40mm). Second, individuals with a short upper lip will show more tooth structure than those with a long upper lip (3.56 vs. 0.59mm). Third, it’s important to know that we show less tooth structure as we age. That is almost always true except in the case of a compensatory eruption, where people may show more tooth structure. For example, an individual under 29 years old will show more than double the upper tooth structure compared to the ages 30-50 (3.37 vs. 1.26mm). It is because we lose the elasticity of the upper lip. It means less of the upper teeth become visible and increased visibility of the lower teeth.

We use phonetic references to check how vertical dimension affects speech: m, s, and v sounds. Repeating the letter M is a good way of determining how much display of the upper teeth is present at rest. This sound puts us very close to our rest position– the vertical dimension of rest. It is an excellent sound to see if the contour of new crowns is appropriate. When saying F and V sounds, you strike your upper incisors on your lower lip when you say these letters. Try saying F and V without touching your incisal edge to your lower lip – it is almost impossible, and you cannot correctly make that sound. This sound clues us into the length of the maxillary incisors and their lingual inclination. In a full mouth reconstruction, we generally want to see that the f and v sounds are fluent and occur by striking the lower lip at the wet-dry line junction. S sounds help us determine whether or not a vertical dimension may be lost. The reason is that the rest position does not change, but as teeth wear and the vertical dimension is lost, the s sounds change.
The next concept we will look at is the 22mm rule. It helps us place teeth anatomically by measuring from the vestibule (*) depth to the tip of the tooth (incisal edge) at 22mm. We also want the incisal edge to strike the wet-dry line during f and v sounds. We use this rule when planning reconstructive dental cases. To use this rule, we must capture an excellent dental impression that shows the vestibule’s depth. This rule shows how much room we may have to fit crowns. It is not an absolute but a starting point to determine a vertical dimension.
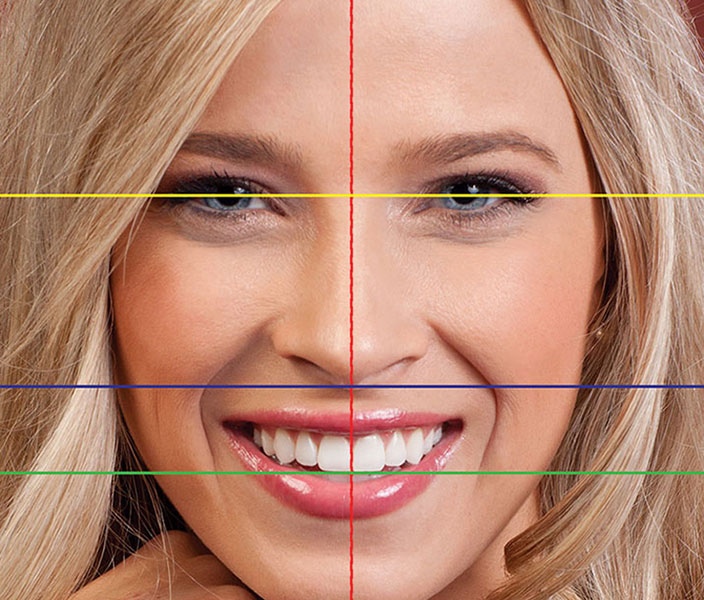
Dr. Hawryluk uses both vertical and horizontal references when assessing the jaw. These are:
- Midline of the face through the midpoint between the eyebrows and the symphysis of the chin.
- Philtrum.
- Bridge of the nose.
Some dentists use the “interpupillary line” as a reference. But, unfortunately, it is not a very accurate horizontal reference. In addition, one eye is higher than the other eye in some patients, so that it would be a terrible reference point.
Assessing how someone smiles can help plan dental rehabilitations. When someone truly smiles, their eyes will move particularly at the corners. However, when patients do not like their teeth, they sometimes hide them with a guarded smile. We can spot a guarded smile if we see no eye movement.
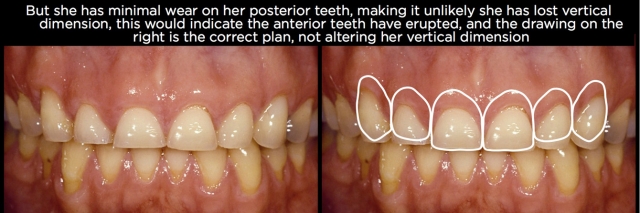
Posterior (not anterior) teeth govern the vertical dimension. Therefore, you will see tones of vertical dimension changes if a patient has lost or worn their posterior teeth. If there is no wear on the back teeth, but the front looks more exposed, this often is compensatory eruption – the front teeth have worn and, consequently, are supra-erupted. We often ask patients to bring us a photo of their biggest smile when they were 20 years old. In cases of compensatory eruption, patients sometimes show less tooth structure when they were 20 compared to years later. However, we wrote earlier that most people show fewer teeth as they age. The only time a patient will show more of their upper anterior teeth with age is in the cases of compensatory eruption. These patients may also develop a “gummy smile”.

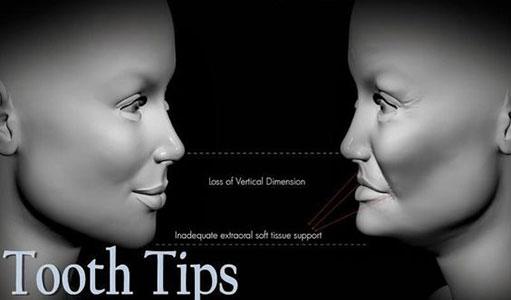
Changes in vertical dimension can modify the face, and its effects can be profound. One interesting study that looked at vertical dimension changes found that 80% of patients who had gone through some form of vertical dimension improvement appeared to be 5-20 younger afterward. (Mohindra, British Dental Journal, 2002). The faces of patients after that can appear longer and narrower.
There is lots of emerging literature about GERD, sleep apnea, and teeth grinding. We used to think that all teeth grinding was parafunctional(*). It is not necessarily the case, and in fact, some teeth grinding is protective- meaning the brain tells the muscles to grind to protect. In sleep apnea, grinding opens the airway, and in GERD, grinding simulates chewing, which causes salivary output with a higher ph.

We hope you have found this article interesting. If you’re looking for a new dentist in Mississauga, please call us!
Glossary
- Condyle: The rounded part mandible that ‘articulates’ with the ‘mandibular fossa’ in the temporal bone.
- Articular eminence: part of the temporal bone on which the condyles slides.
- Cementoenamel junction: the anatomic boundary between the crown and root surface of a tooth.
- Class I occlusion: The most common way upper and lower teeth relate together.
- Vestibule: the fold of tissue between the cheek and bones surrounding teeth.
- Parafunctional: the habitual exercise of a body part in a way other than the most common use of that body part.
Reference:
https://vivalearning.com/member/classroom.asp?x_classID=4330

- Sleep Dentistry: Enhancing Comfort and Care During Dental Procedures - July 11, 2024
- The Revolutionary Injection Molding Technique for Composite Veneers - June 27, 2024
- Why Are Third Molars Called “Wisdom Teeth”? - June 19, 2024