Tylenol and Non-steroidal anti-inflammatory drugs (NSAIDs) are analgesics (pain relievers). However, Tylenol is not an NSAID.
These two drugs have different mechanisms of action in the body. NSAIDs (Non-steroidal anti-inflammatory drugs) are medications that target mainly three underlying processes:
- Analgesic (they decrease pain).
- Antipyretic (they reduce fever).
- Anti-inflammatory (they reduce inflammation).
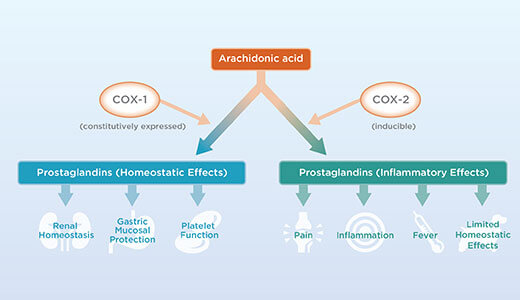
They do so by inhibiting cyclooxygenases (*). The cyclooxygenase isoforms are called COX1, COX2, and COX3.
COX1 is constitutively expressed and is physiological. It offers gastric (stomach) protection, aids in platelet (blood cells) aggregation, and helps maintain the salt/water balance in the kidneys. COX2 is not physiologic and is induced only in the presence of inflammation. Its activation results in increased prostaglandins, which help mediate pain and inflammation. COX3 is a minor variant of the COX1 gene, constitutively expressed in the brain. It offers central regulation of pain and fever in the brain and prostacyclin synthesis.
Aspirin and Ibuprofen are non-selective COX inhibitors and will inhibit COX2 and COX1. As a result, they increase the risk of gastric damage, prevent platelet aggregation, and prevent the normal excretion of sodium in the kidney. Examples of non-selective COX inhibitors are Ibuprofen, naproxen, and acetylsalicylic acid.
There are some adverse effects of aspirin.
- Hypersensitivity. About 5% of the population has an intolerance to Aspirin. It is increased to about 20% in asthmatic patients. 1% of people have a true aspirin allergy. there are cross allergies to foods containing salicylates and tartrazine.
- Tinnitus, headaches, nausea, vomiting: reversal can be in 2-3 days after modifying does or stopping the drug.
- Renal function: on large does greater than 4 grams can cause renal failure.
- Aspirin can decrease platelet aggregation, which increases bleeding time.
- You should avoid aspirin in the last trimester of pregnancy as it is associated with low birth weight, prolonged labor, and increased blood loss during pregnancy.
- Asprin can be associated with gastric ulcers.
- In the endocrine system, very high levels of aspirin can increase corticosteroid synthesis, which decreases thyroid activity.
Selective cox2 inhibitors will focus on limited inflammation and do not cause blood clotting or kidney function issues. In early COX2 inhibitor medications, there was an increased risk of dying from a heart attack – the reasons are still unclear. The true selective cox2 inhibitors such as Vioxx are not in the Canadian market anymore. Available drugs such as celecoxib and meloxicam do inhibit COX 1 to a minor extent -but focus on COX 2.

If your doctor gives NSAIDs in conjunction with Aspirin, you don’t get increased bleeding because NSAIDS and Aspirin compete for the same target in platelets. However, one difference between NSAIDS and Aspirin is an irreversible inhibitor – any molecule it binds to will be out of commission forever. As a result, platelets inhibited by aspirin will no longer be able to recover and aggregate. On the other hand, non-selective NSAIDs are not irreversible inhibitors – even though their mechanism of action is the same as aspirin. If you give Aspirin and NSAIDS together, the NSAIDS will block the cardioprotective effect of Aspirin and increase the risk of thromboembolism. If a patient is already taking aspirin for cardiovascular protection, your doctor may administer them 30-120 mins after ASA (and not together) to avoid complications.
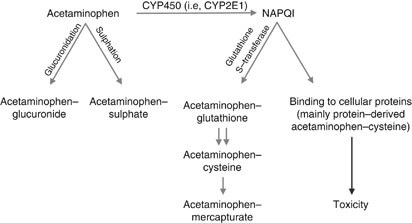
Acetaminophen is a funny drug in that it is not an opioid but also not an NSAID. Acetaminophen has no anti-inflammatory properties. It has a low affinity for COX1 and 2. However, it has a high affinity for the reversible inhibition of COX3 in the brain. Understanding the mechanism of action of acetaminophen is essential, and it is a myth that it is an entirely safe drug. 95% of the metabolism is in the liver through “glucuronidation” and “sulfation” processes. Elimination of the conjugated metabolite is thru the urine. Cytochrome p450 metabolizes a small amount to form NAPQ1– which is highly reactive. It is a highly toxic substance to the liver and kills liver cells. Usually, it binds quickly to glutathione which neutralizes it. The problem is some individuals have limited capacity for glucuronidation and sulfation– such as those with liver pathology. Acetaminophen is the most common cause of drug-induced liver failure in North America. Maximum doses of acetaminophen (in general) are 4000mg per day if under 65 and 2600mg per day if over 65. The pediatric patient should not exceed 75mg/kg/day (not to exceed 4g per day).
We hope you have enjoyed our article – thank you for reading it!
Glossary:
- Cyclooxygenase – enzyme that catalyzes the conversion of arachidonic acid to prostaglandins.
Reference:
Utooth.ca: Pain Management in Dentistry, Myths and Evidence-Based Practice, Lanca. 2022
Birth Injuiry Center: Tylenol Link to ADHD & Autism

- Understanding Dental Cupping on Molars: Causes, Prevention, and Treatment - August 14, 2024
- Bone Preservation: Essential for Strong Dental Implants - August 5, 2024
- Porcelain Veneers from Design to Finish - July 27, 2024